
AT AAIC 2016
TORONTO (FRONTLINE MEDICAL NEWS) – Patients with amnestic mild cognitive impairment made significantly more errors during a complex test of driving skills and showed altered brain activity while performing this test in a two-part study.
The findings are the first to show a correlation between physiologic brain activity and driving and suggest that patients with mild cognitive impairment (MCI) may already be experiencing potentially dangerous changes in their ability to operate a motor vehicle, Megan Hird said at the Alzheimer’s Association International Conference 2016.
“Driving is a highly complex behavior that requires the integration of cognitive, motor function, and perceptual abilities,” said Ms. Hird, a researcher at the University of Toronto. “Individuals with multidomain MCI can express memory, visuospatial, and executive function deficits” even before their less demanding activities of daily living are affected. Nevertheless, Ms. Hird said, “these deficits can affect someone’s ability to drive safely.”
The decision to hang up the car keys is always a tough one for patients with dementia, their families, and their physicians, and there are no guidelines in the United States or Canada to help in that decision. But Ms. Hird and her colleagues recently published a meta-analysis of driving studies in which patients with very mild Alzheimer’s were 10 times more likely to fail an on-road driving test than were cognitively healthy drivers ( J Alz Dis. 2016;53[2]:713-29 ).
Nevertheless, both the American and Canadian Medical Associations state that a diagnosis of cognitive impairment is not sufficient to withdraw driving privileges, and no cognitive test is capable of determining driving ability.
Ms. Hird used a combination of a driving simulator and functional MRI to study driving skill and the neural correlates of that activity. There were two parts to the study. The first comprised 20 healthy controls and 24 amnestic MCI patients (11 with single-domain MCI and 13 with multidomain MCI). The driving tasks were routine right and left turns, plus left turns against traffic and left turns against traffic with auditory distraction.
Overall, those with MCI (both single- and multi-domain patients combined) committed significantly more risky driving errors than the control group (mean of 9 vs. 3). Risky errors were considered errors that could result in an imminent collision, crossing the center line into oncoming traffic, or crossing onto the sidewalk.
When the researchers examined the MCI groups separately, they determined that only those with multi-domain MCI performed significantly worse than did controls (mean of 14 vs. 2.7 errors). These errors were most often committed during the more complicated left turns. There were no significant between-group differences in routine right and left turns.
Differences in brain activation revealed
The second part comprised 32 patients: 16 with MCI and 16 age-matched, cognitively normal controls. These subjects undertook both the driving simulation and the functional MRI test.
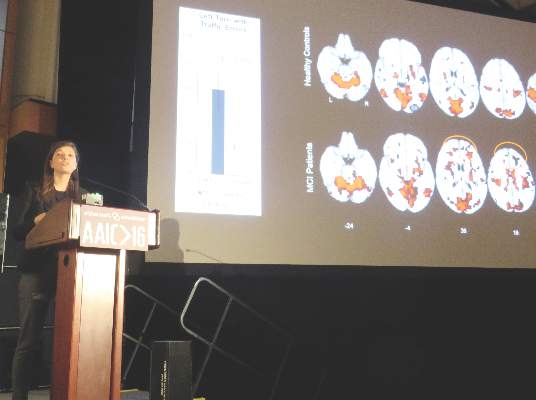
On the uncomplicated right turns, there were no between-group differences in errors, Ms. Hird said. However, there were some differences in the way the subjects’ brains reacted to the task. “On the brain activation patterns, the healthy controls showed some negative activation in the temporal and occipital regions, areas that actually were activated in the patients. The patients also showed some increased signal in the posterior medial regions, compared with the healthy controls. Overall, however, the activation patterns looked quite similar between the two groups.”
The left turn into traffic task showed quite different results. “In the MCI group, there was more anterior activation. They also showed significantly higher activation than did the control group in the orbitofrontal, medial superior, and midfrontal cortex – all of which are involved in planning, higher-order attention, and cognitive control.”
Recognizing that there are demonstrable differences in brain activation that correlate with poor driving performance could spark the creation of an objective clinical measurement tool for determining driving status, Ms. Hird said.
“This is an important fundamental step in the development of a tool that is sensitive and specific for addressing the driving safety of these patients.”
During discussion after her presentation, she fielded a question from an Australian clinician, who said his country likewise has no objective measure of when driving is no longer safe for a dementia patient.
“We accept the fact that people do drive with some degree of cognitive impairment,” said the physician, who did not identify himself. “But there are regions where having a license is important for social engagement. And we know that social disengagement drives rapid progression of cognitive decline. I think there is a real tension here between the withdrawal of licensure and the preservation of social engagement.”
Ms. Hird agreed. “Obviously, many MCI patients do retain the ability to drive safely. But we need to achieve a balance between maintaining patient autonomy and the safety of the general public.”
Ms. Hird had no financial disclosures.
On Twitter @alz_gal



