Even though more patients are taking a proactive role in learning about their disease and treatment options, adherence rates are still down. It is up to marketers to ensure that patients are getting the best information—and are not getting lost in the sea of endless sources and opinions.
Recent Internet joke: What would a person from the past say if he knew you had an electronic device that could access nearly all of human knowledge…and you used it to start arguments with idiots and send your friends pictures of cats?
He might be even more shocked to find that you also use it to dig up information that contradicts your doctor’s orders.
What’s going on here? Consider:
• Nearly 50% of patients are non-compliant in taking their medication.
• Over one-third of adults in the U.S. are obese and the rate is growing.
• The rate of adults getting a colorectal screening is declining among an aging audience.
• Only one-third of adults report routinely applying sunscreen when out in the sun for extended periods of time, in spite of the growing prevalence of skin cancer.
Why are adults not taking better care of themselves, especially when their health is at stake?
Q: Why do men die younger?
A: They won’t ask for directions.
Doctor: What’s the problem, Jack?
Patient: Ah, nothing. Just need to get back in the gym.
D: You mean you want to lose weight?
P: Yeah, that mostly.
D: “Mostly.” There’s something else?
P: Not important.
D: Maybe it’s something you should talk to me about.
P: Doc, if I thought you could do anything, I’d tell you about it.
Typical man, right? Has a problem, but is too male to come right out and ask for help.
Research tells us that women will open up to their physicians (male or female) more often than men will. It’s true that women are more proactive about managing their health, but it goes beyond that. Men just tough it out. A U.K. study found that 31% of men don’t seek help even for life-threatening conditions—because they’re “embarrassed.”1 Embarrassed to keep living?
Men think “If I ignore the problem, it doesn’t exist,” notes Carolyn Leighton, a pharmaceutical veteran with past experience in marketing to males. She has seen males go to extreme lengths to avoid treatment for conditions that are seriously affecting their lives. “Men tend to be scared of what’s wrong.”
How do we—and healthcare providers—do something about this?
Some pointers:
• A 1990 study by the American Medical Association showed that fear, denial, embarrassment and protecting their masculinity were the main reasons males did not routinely visit a doctor.2
• A German study looked at factors that drove males to initiate a discussion around erectile dysfunction (ED). Given written material on a condition, they were 38% more likely to discuss their treatment with the doctor.3
• Psychological Science published a study that concluded males are more likely to talk to their physician about a medical condition if they think many other men are discussing it.4 (The opposite is true, too: if they don’t think guys are talking about it, they’ll avoid it.)
To drive action, we must show (male) patients they are not alone, educate them on how their disease burdens them, and focus on the aspirational aspects of treatment. Contrast this to the approach used with female-oriented Overactive Bladder (OAB) marketing. With OAB, the focus is on the burden of the disease. With ED, it’s on the hero who is already on therapy. The different approaches are based on how male and female patients differ in thinking about health and prescription therapy. This shows a clear distinction in how to educate and the role prescription treatment plays. And that’s just a microcosm of the bigger disconnect between physicians and patients.
Doctor’s Orders? Or Doctor’s Suggestions?
In 2011, the Mayo Clinic examined the rate of patient medication adherence in Sweden for 24 months following an ischemic stroke. By two years post-event, compliance rates dropped to as low as 50–80%, despite patients having experienced an event that could have rendered them severely incapacitated or dead.5 (See Figure 1).
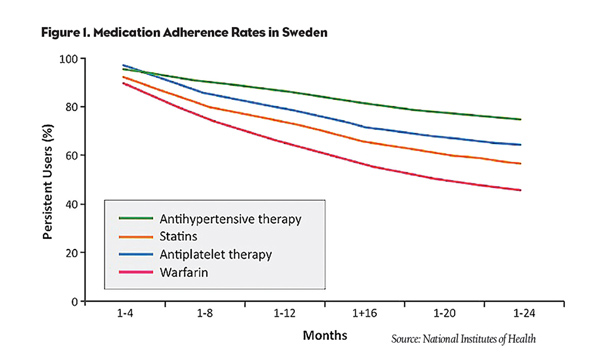
Is this an education problem? A motivational problem? An economic/access problem? Probably a combination.
Patients in the U.S. are often discharged with a diagnosis, a prescription and little else in terms of guidance. Before they get to the pharmacy, many will research the medication online. And we know where that leads: To a stew of good, bad and indifferent data, and a high risk that the patient won’t be able to tell one type of information from the other. Some even decide to develop their own treatment plan. Doctors, in turn, find themselves explaining preventive steps patients can take…and then being ignored. Or they tone down the severity of the illness for fear of scaring the patients out of their wits. What can we as marketers do to effect a shift in consumer behaviors?
It’s Really This Bad
A recent article in Nursing Times points out that “old models of passive patients complying with ‘doctor’s orders’ no longer apply, as patients are now given increased choice over when, where, and how they are treated.”6 A 2009 report by the Pew Internet Trust revealed that 56% of people have “changed their overall approach to maintaining their health or the health of someone they help take care of” because of something they read online.7
Do patients often trust rumor-style advice over credible, validated, info? Yes. One study found that patients feel information obtained by “word of mouth” about a pharmaceutical product is “believable/credible” in nearly seven out of 10 discussions.8 Social media, in particular, has exponentially increased the number of conversations occurring. More and more patients are convincing themselves and others to recklessly abandon treatment altogether.
But It Can Be This Good
We can no longer assume that the traditional linear marketing framework we’re accustomed to still applies. We have a perfect storm of runaway “information,” DTC marketing and an increasing number of chronically ill people. It is essential that we understand who the influencers are in their lives and where they exert the greatest sway.
Trust the research: In launching a brand, an extensive amount of time and research is compiled on patients, their interactions with doctors and the marketplace. We use that data to break into the market and drive brand adoption. Then we start to realize we’re facing an adherence problem, and we ditch the research we’d conducted only a few short years ago. We should ensure that each brand planning cycle involves a thorough review of existing research so as to not lose sight of these valued learnings.
Give them the data they need: If a brand’s mechanism of action is simple enough for the average patient to understand, do we need to overly communicate how the product works in an RM program? Or do we need to dispel concerns about the safety of the product that appeared online, or were implied in a competitor’s marketing? Narrow the focus of the communication to what the consumer needs from you.
Monitor and correct: The simple social strategy of just responding to what your customers are saying/reading is easy to implement, in a regulatory-compliant manner. A 2011 study among Online Health Activists presented to the FDA revealed that nearly two-thirds of people actively searching for health information in the social space expect healthcare organizations to “get involved in monitoring and correcting misconceptions or misinformation about their product anywhere on the Internet.”9 We have a responsibility to monitor the prevailing sentiment in the social space and respond to it through compliant channels, such as email or their brand site.
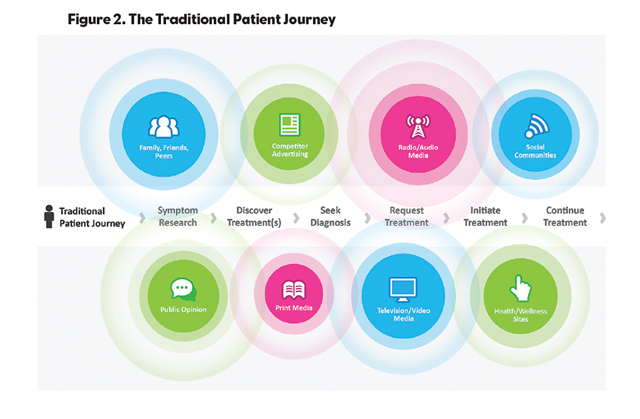
Find your consumers: Start examining how and where consumers interact and learn about the realities of your brand or the disinformation. Yes, patients do go through the exercise of evaluating symptoms, exploring treatments, getting diagnosed, asking for a treatment and treating their condition (see Figure 2). However, the process of evaluation is ongoing, and we have a duty to be present during key interception points to provide a credible answer to their concerns; this includes giving the doctors and allied health professionals the information they need to work with patients to proactively manage patient concerns.
Be there: “We’re seeing compliance challenges in categories as severe as angina, breast cancer and HIV,” remarks Jim Curtis, Chief Revenue Officer at Remedy Health. To address these challenges, Remedy Health has been developing solutions that take a holistic approach to helping patients be more adherent. Specifically, this requires a brand having a presence:
• at the point of care; immediately upon leaving a doctor’s office;
• at the pharmacy;
• and even at home or work, through a combination of traditional media (e.g., in-office guides) and technology (email, mobile, etc.).
Mr. Curtis further noted, “When we’ve used technology on the consumers’ terms, by allowing them to select how they want to engage with us, we’ve seen that we’ve been able to affect improved patient adherence.” In one partnership, Remedy developed an adherence tool for a major health insurance provider that allowed users to set up medication reminders, resulting in an estimated savings of $6MM in reduced emergency care.
We want patients to be armed with the best information available, to have educated discussions with physicians, in an effort to steer patients and prescribers towards trustworthy brands. With the right attention to the right information in the right places, we can do this.
References:
1. Science Daily; July 27, 2010, “Few People Are Doing It, So Why Should I? Motivating Men to Seek Cancer Screening.” http://www.sciencedaily.com/releases/2010/07/100727112837.htm
2. South Source, June 6, 2011, “Men & Health: The root of male health issues.” http://source.southuniversity.edu/men-and-health-the-root-of-male-health-issues-43917.aspx
3. International Journal of Impotence Research; June 19, 2007, “Can written information material help to increase treatment motivation in patients with erectile dysfunction?” http://www.ncbi.nlm.nih.gov/pubmed/17304205
4. St. Petersburg Times; December 28, 2010, “If men resist seeing a doctor, try these arguments.” http://www.eastvalleytribune.com/local/health/article_255b08e0-123e-11e0-a790-001cc4c03286.html
5. National Institutes of Health, April, 2011, “Medication Adherence: WHO Cares?” http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3068890/
6. Nursing Times, December 7, 2012, Improving Drug-Concordance in Patients with Chronic Conditions. http://www.nursingtimes.net/Journals/2012/12/07/o/c/t/040615Improving-drug-concordance-in-patients-with-chronic-conditions.pdf
7. Pew Internet Trust, June, 2009, “The Social Life of Health Information.” http://pewinternet.org/~/media//Files/Reports/2009/PIP_Health_2009.pdf
8. Keller Fay Group, June 10, 2008, “Unleashing the Power of Word of Mouth: Where DTC Meets C2C.” http://www.docstoc.com/docs/976056/Unleashing-the-Power-of-the-Word-of-Mouth
9. WeGo Health, DTC National Conference, April 7, 2011, “Social Media Won’t Wait: Health Activists Speak Out, Industry Speaks Up.”