
Various theories abound regarding how people make decisions, but at the end of the day they are all just theories. Until we can climb into people’s heads, we have to rely on psychological theory as a way to explain and understand what’s going on so that we can motivate our target market into taking desired actions. After all, we need to know where patients are mentally before we can take them where we want them to go.
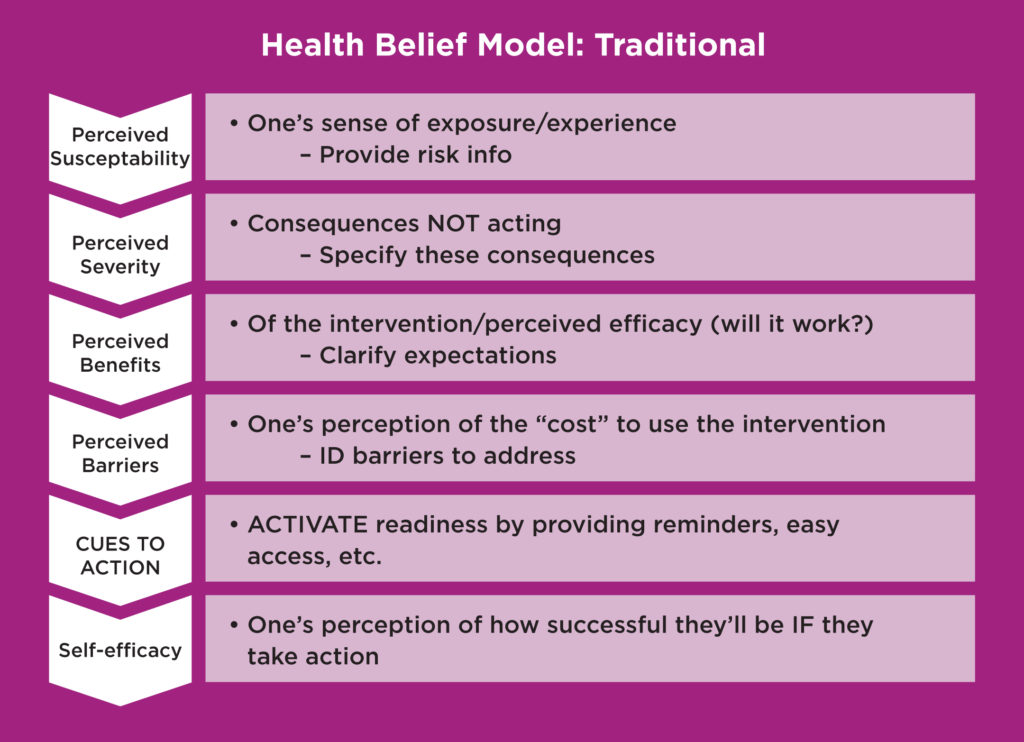
For many years, the HBM (Health Belief Model, Figure 1) has been a popular “rational” framework for healthcare research. It involves asking a handful of key questions to determine whether individuals would be likely to make a particular health choice. To apply HBM in market research, we might determine where the main roadblocks are in respondents’ thought processes and what messaging might help them overcome an obstacle or spur them to take action, for example1:
- One’s perception of how “at risk” a person feels for getting the condition (i.e., feelings of susceptibility)
- One’s perception of severity
- What would it be like to have or to contract this condition?
- One’s perceived benefits of doing the intervention or behavior
- How effective would it be?
- One’s perceived barriers
- What are the negatives of doing the intervention or behavior?
- Cues to action (e.g., ads, PSAs, HCP recommendations, having symptoms)
- Self-efficacy: One’s belief in their ability to take the necessary action
Figure 1. Traditional Health Belief Model
 Of course, other demographic or psychosocial variables can also affect these perceptions (e.g., level of education, social class, ethnicity). Nonetheless, in real-world market research, we might ask variants of these questions to understand how likely at-risk respondents are to make the decision to get screened (for diabetes, for example), and go from there.
Of course, other demographic or psychosocial variables can also affect these perceptions (e.g., level of education, social class, ethnicity). Nonetheless, in real-world market research, we might ask variants of these questions to understand how likely at-risk respondents are to make the decision to get screened (for diabetes, for example), and go from there.
HBM’s Limitations
However, there are limitations to HBM. It does not account for things like “habitual health-related behaviors” such as smoking, which may become relatively independent of the conscious health-related decision making process2; nor are the relationships between these variables spelled out in clear rules of combination, but it’s assumed that they have an additive effect.
In sum, “the HBM views health behavior change based on a rational appraisal of the balance between the barriers to and benefits of action.”3
Underlying Emotions Drive Engagement
But, since it’s understood that underlying emotions help people identify with or relate to a brand, more pharmaceutical companies are using emotional drivers to position or promote their brands. So in addition to our rational side, the prevailing belief for some years now is that underlying emotions are what truly drive our decision-making (outside of payer/cost restrictions). But in fact, it’s now believed that decision making is >80% subconscious—including social/peer influence.
Enter Behavioral Economics (BE)
BE began as a theory about how people make financial decisions but has since expanded and been applied to other areas, such as healthcare. BE proposes that humans essentially have two thought systems:
- A quick-paced System 1 thought process (based on past experience as well as the use of subconscious mental shortcuts or rules called “heuristics”).
- The more “logical” (conscious) System 2, which is slower and relies on information to guide decisions.
While it’s been postulated that System 1 frequently overrides System 2—even in the presence of actual information—I’m not quite ready to throw the baby out with the bathwater.
In my humble opinion, traditional research methods (that involve asking respondents what they think) are still of value, particularly when people are making novel or “hard” decisions. For example, it’s possible that System 2 thinking (which entails more effort) may garner a slightly higher or lesser proportion in some situations than it does in others.
Though we often hear about the “80/20 rule” that skews in favor of emotional drivers, it stands to reason that these proportions likely shift in weight depending on whether one is deciding on something as inconsequential as picking out shoes to wear versus whether to start on a particular medication (though I agree there’s obviously a large emotional element to the latter). For argument’s sake, let’s say that psychologists find a way to prove that decisions are actually 100% emotional—as some already believe. There are still times when we need to quantify behaviors (e.g., to ask whether a person of a certain age has ever been vaccinated for shingles), for which it’s generally acceptable to take stated answers at face-value or as fact.
Though some believe that, in this fast-paced world, even more of our “important” decisions are being relegated to our System 1 thinking, in the ideal research situation, when feasible we should still consider using methodologies appropriate to accessing both systems.
Uncovering Underlying Emotions
At PulseCX, in addition to recommending primary research where interviewing techniques like laddering, projection, etc., can uncover emotional drivers, we first like to conduct internal secondary research to assess these drivers. This assessment is accomplished through “social scraping,” (Figure 2) which involves a review of online forums to see how patients with a particular condition are feeling without being asked outright. These sites may also shed light on how patients are being subtly influenced by their peers via what they’re reading online.
Figure 2. “Social Scaping”
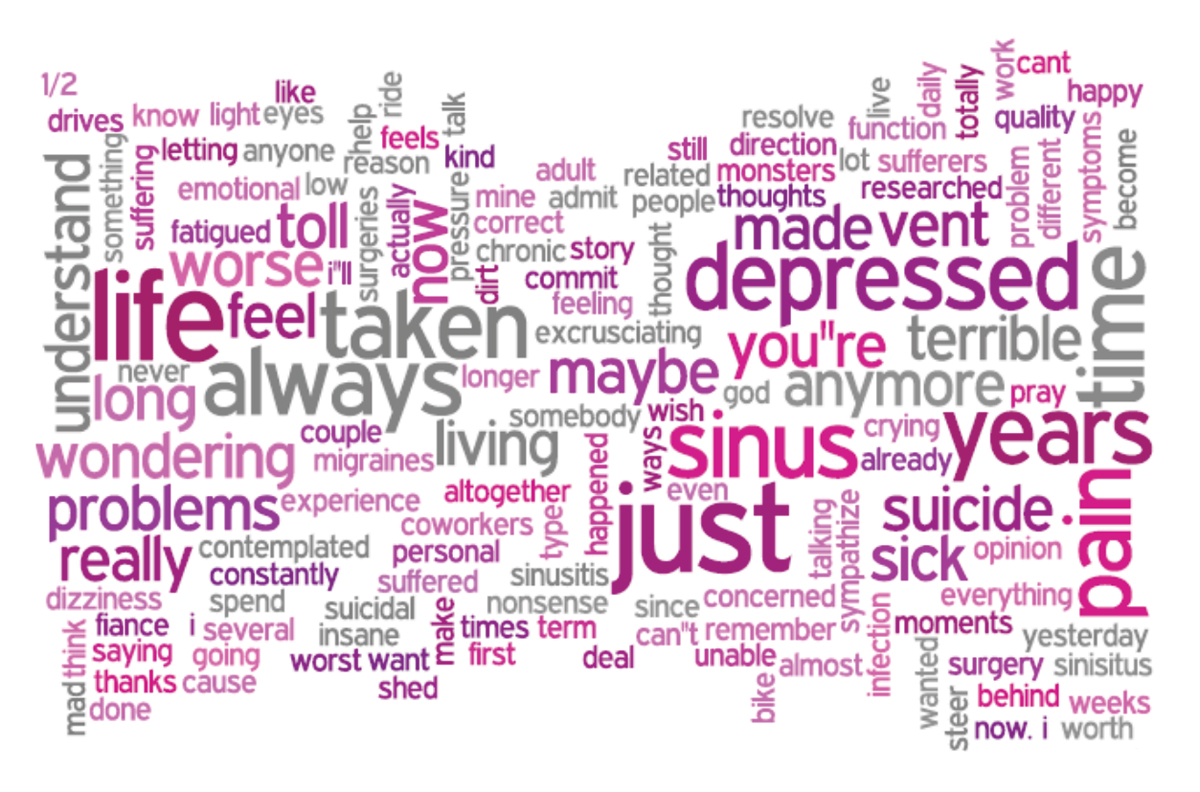 Additionally, imagery posted on sites like Tumblr also give us a good sense of what it’s like to have a particular condition, and so can be invaluable in developing concepts that reflect how patients may be feeling emotionally and physically (Figure 3).
Additionally, imagery posted on sites like Tumblr also give us a good sense of what it’s like to have a particular condition, and so can be invaluable in developing concepts that reflect how patients may be feeling emotionally and physically (Figure 3).
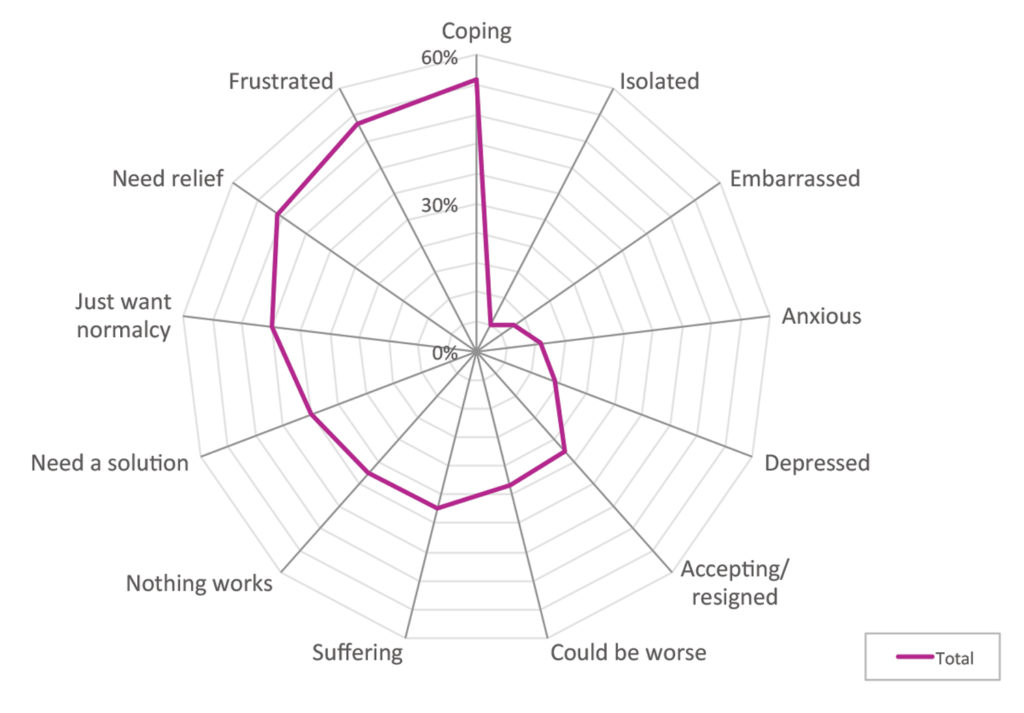
Figure 3. Tumblr’s Patient Coping Insights
 Charting the Emotional Drivers
Charting the Emotional Drivers
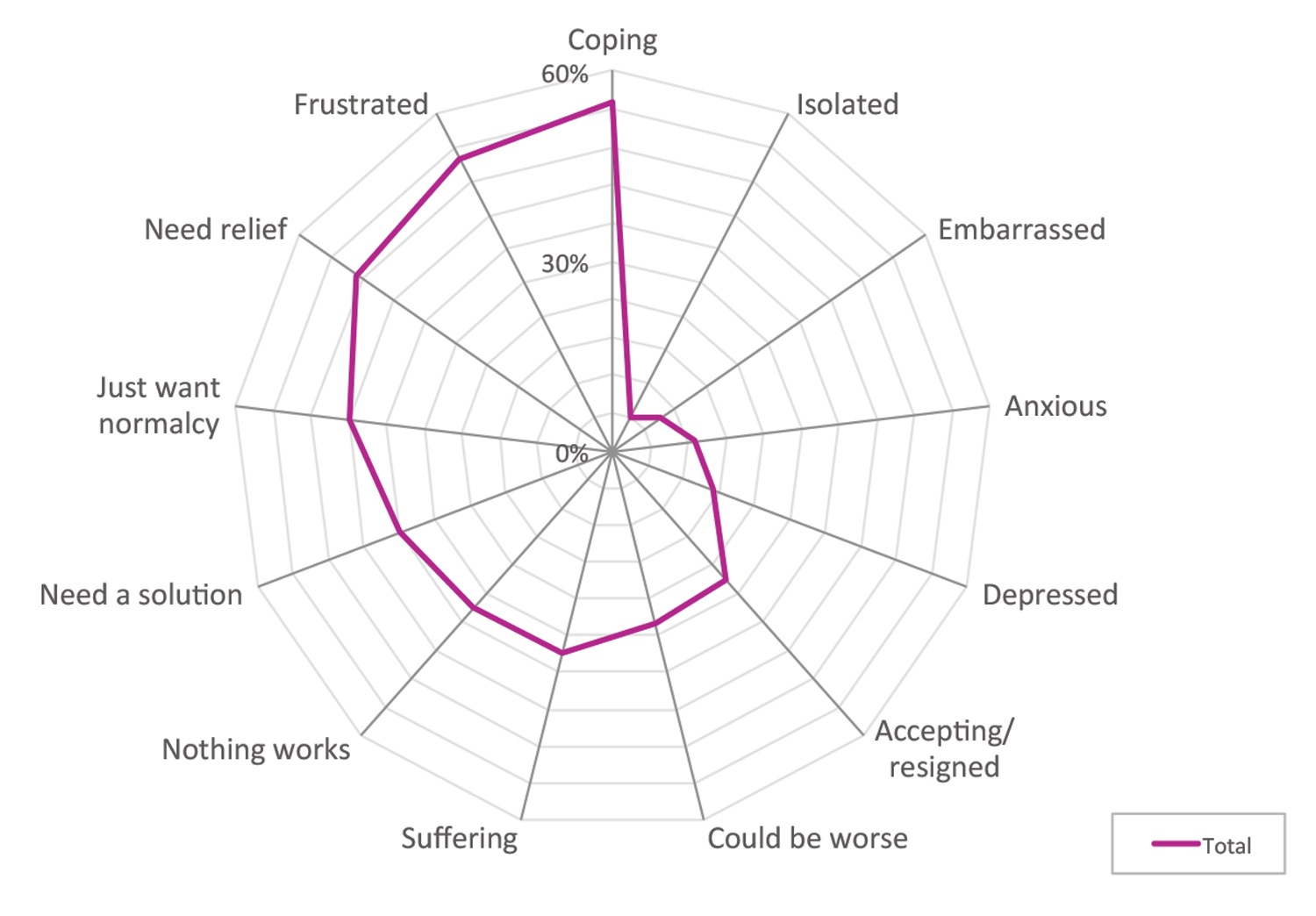
One example of how we gathered both emotional insights as well as more conscious patient thoughts is demonstrated through work we’ve done in CRS (chronic sinusitis). First, we scanned online forums to get an idea of what CRS is like from the patient perspective, and were shocked to find talk of depression and even suicide.
This data was then used to inform our quantitative questionnaire design since we then knew which emotions/attitudes to include to determine what the majority of patients thought about their condition. Our goal was to uncover not just patient emotions and attitudes towards their CRS, but also corresponding prevalences.
In addition, to determine what proportion would be more likely to take the next step and inquire about a procedure involving our client’s product, we had them assess key issues that were loosely based on the HBM, including:
- The severity of their condition and life impact
- Treatments tried and barriers to (surgical) treatments
- Perceived benefits of an in-office procedure
- Concerns if left CRS untreated
- What it would mean to find relief, etc.
Insights gathered from both phases were then used to develop a patient journey map (e.g., what the bulk of patients are likely thinking, feeling, and doing at different stages).
inVibe: Something New in the Tool Chest
A newer (and relatively inexpensive) approach is now available to us through a strategic partner, inVibe (voice-powered healthcare insights on demand), which allows us to measure subconscious emotions using voice assessment.
While speech emotion analytics have multiple applications, their most obvious use is for quick ad concept testing and to better understand the emotions behind overt (or conscious) responses. Through the inVibe technology platform, we can field these mini-qualitative projects very quickly with patients and/or HCPs (<1 week).
How It Works
Via audiotaped responses to a handful of written questions presented online to panel members via inVibe’s proprietary software, we can assess the proportion of respondents whose underlying emotion is, say, sadness or joy in response to a particular question.
In essence, we can capture and assess five underlying emotions, as well as positive or negative sentiment (based on respondent tones and words used, respectively), that are associated with short, 13-second audio clips (or sections) of each respondent’s verbatim. Via our analysis, we can then tie these reactions back to what they were actually saying during each clip. These results, in turn, feed our understanding as to which of their own words evoke certain (good or bad) emotions for use in campaign development.
Where Do We Go From Here?
Theories abound about how humans think. The HBM takes a more rational approach, while BE argues that decisions are based largely on emotions. How do we use this knowledge in a practical way to inform our end deliverables? How do we uncover what the patient experience is like so we can help them in their journey to reach their goals?
Regardless of your current stance on the emotional versus logical driver debate, your best approach is to use methodologies that address both systems of thought (Figure 4). Whether it’s the emotional drivers you uncover through social scraping and the inVibe platform, or the conscious thoughts gathered through more traditional means, both will provide the insights necessary to truly define the customer experience (CX) and develop communications that engage and drive behavioral change.
Figure 4. Rational and Emotional Components of Decision Making
References:
- University of Twente; https://www.utwente.nl/en/bms/communication-theories/sorted-by-cluster/Health%20Communication/Health_Belief_Model.
- “The Health Belief Model: A Decade Later.” Nancy K. Janz, RN, MS, Marshall H. Becker, PhD, MP. Health Education & Behavior, March 1, 1984, BMC Public Health. 2007; 7: 104.
- “A Review of Health Behaviour Theories: How Useful are These for Developing Interventions to Promote Long-term Medication Adherence for TB and HIV/AIDS?” Published online 2007 Jun 11. doi: 10.1186/1471-2458-7-104.