Among a large cohort of patients referred for endoscopy for suspected celiac disease as well as all upper gastrointestinal symptoms, a single additional D1 biopsy specimen from any site significantly increased the diagnostic yield for celiac disease, according to researchers.
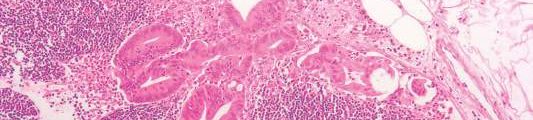
Of 1,378 patients who had D2 and D1 biopsy specimens taken, 268 were newly diagnosed with celiac disease, and 26 had villous atrophy confined to D1, defined as ultrashort celiac disease (USCD). Compared with a standard D2 biopsy, an additional D1 biopsy increased the diagnostic yield by 9.7% (P less than .0001). Among the 26 diagnosed with USCD, 7 had normal D2 biopsy specimens, and 4 others had negative tests for endomysial antibodies (EMAs), totaling 11 patients for whom celiac disease would have been missed in the absence of a D1 biopsy.
“The addition of a D1 biopsy specimen to diagnose celiac disease may reduce the known delay in diagnosis that many patients with celiac disease experience. This may allow earlier institution of a gluten-free diet, potentially prevent nutritional deficiencies, and reduce the symptomatic burden of celiac disease,” wrote Dr. Peter Mooney of Royal Hallamshire Hospital, Sheffield, England, and his colleagues. (Gastroenterology 2016 April 7. doi: 10.1053/j-gastro.2016.01.029).
The prospective study recruited 1,378 consecutive patients referred to a single teaching hospital for endoscopy from 2008 to 2014. In total, 268 were newly diagnosed with celiac disease, and 26 were diagnosed with USCD.
To investigate the optimal site for targeted D1 sampling, 171 patients underwent quadrantic D1 biopsy, 61 of whom were diagnosed with celiac disease. Biopsy specimens from any topographical area resulted in high sensitivity, a fact that increases the feasibility of a D1 biopsy policy, since no specific target area is required, according to the researchers. Nonceliac abnormalities such as peptic duodenitis or gastric heterotopia have been suggested to impede interpretation of D1 biopsies, but these were rare in the study and did not interfere with the analysis.
USCD may be an early form of conventional celiac disease, an idea supported by the findings. Compared with patients diagnosed with conventional celiac disease, patients diagnosed with USCD were younger and had a much lower rate of diarrhea, which by decision-tree analysis was the single factor discriminating between the two groups. Compared with healthy controls, individuals with conventional celiac disease, but not USCD, were more likely to present with anemia, diarrhea, a family history of celiac disease, lethargy, and osteoporosis. Patients with USCD and conventional disease had similar rates of IgA tissue transglutaminase antibodies (tTG), but USCD patients had lower titers (P less than .001). The USCD group also had fewer ferritin and folate deficiencies.
The researchers suggested that clinical phenotypic differences may be due to minimal loss of absorptive capacity associated with a short segment of villous atrophy. Given the younger average age at diagnosis of USCD and lower tTG titers, USCD may represent an early stage of celiac disease, resulting in fewer nutritional deficiencies observed because of a shorter lead time to diagnosis.
Although USCD patients had a milder clinical phenotype, which has raised concerns that a strict gluten-free diet may be unnecessary, follow-up data demonstrated that a gluten-free diet produced improvement in symptoms and a significant decrease in the tTG titer. These results may indicate that the immune cascade was switched off, according to the researchers, and that early diagnosis may present a unique opportunity to prevent further micronutrient deficiency.
Dr. Mooney and his coauthors reported having no relevant financial disclosures.
ginews@gastro.org